


From GAZEL to CONSTANCES: The Construction of an Open General-Purpose Longitudinal Epidemiological Laboratory
Mercel Goldberg
Marie Zins
Public Health and Epidemiology of Occupational and Social Determinants of Health
1. The Context of Longitudinal Cohorts in Epidemiology: A Necessary Research tool
Epidemiology faces many problems where time plays an important role at an individual or a population scale. The temporal sequence between exposure of subjects to putative risk factors and health outcomes must be taken into account to study the risk of developing diseases, the latency periods between exposure and the onset of disease, or to analyze the evolution of a disease after it occurred. Modeling the sequence and interactions between personal and environmental factors and the health status or the incidence of various health outcomes is often necessary to understand the complex pathways leading to disease. When analyzing evolutions in the pattern of diseases or mortality in populations, one has to disentangle the relationships between age and generation or period effects to have a clear understanding of the changes that occurred over time.
The longitudinal cohort design, i.e. individual follow-up over time of subjects, is theoretically the best method for dealing with these methodological problems. It also allows for the prospective collection of adequate data at an individual level, thus avoiding some major biases [Szklo, 1998].
In the domain of public health and medical research, two main types of epidemiological cohorts exist: large longitudinal representative samples and longitudinal cohorts of volunteers. Large longitudinal representative samples of the whole population allow for the description and quantification of health problems at the population level, and for the analysis of changes over time. The necessity of representativeness implies that subjects are anonymously included in these cohorts, and do notactively participate in the follow-up, which is usually performed through the linkage with national data bases, such as employment, taxes, or causes of death registers. On the other hand, cohorts of volunteers allow for the collection of more specific data directly from the subjects, such as lifestyle factors, working conditions, social activities and relationships, biological samples or various health scales. In a search for causality, such data are needed to understand the mechanisms linking different conditions and exposures and the occurrence of health problems. However, relying on the voluntary participation of the subjects always implies some amount of selection effects associated with socioeconomic, demographic, occupational and health factors [Goldberg et al, 2001], and cohorts of volunteers can not be representative of the whole population. Another aspect of the difference between these two types of cohorts is the size of the samples: general population samples are usually much larger than cohorts of volunteers, because the collection of additional personal data during long period of follow-up can be very costly.
Some recent work on social inequalities and social determinants of cancer in our Inserm research unit illustrates these complementary aspects. Using a large representative sample of about1% of the French population constructed from successive censuses, we were able to describe the differences in cancer mortality according to occupational categories and education level and to demonstrate and quantify the widening of social inequalities in France over a period of 15years [Menvielle et al., 2005]. Working within the much smaller GAZEL cohort, where numerous personal data are collected over more than 15years, we were able to analyze the contribution of specific health behaviors and other risk factors (age, marital status, tobacco and alcohol consumption, weight, diet, asbestos exposure, family history of cancer, and reproductive history) to the social gradient in cancer incidence [Melchior et al., 2005].
As epidemiologists, our main interest is in understanding health mechanisms; therefore we will restrict the remainder of this paper to the scope of longitudinal cohorts of volunteers.
1.1. A complex research tool
Cohorts of volunteers are a long term practice in epidemiology, some of them following-up now the same groups of individuals for more than 50 years. Yet, they pose difficult organizational, technical and funding problems, mainly due to the long term aspect of these cohorts. Specifically, some of these are detailed below:
- Size: most of the existing cohorts are restricted in sample size, and analyzing rare events in specific groups may lack power.
- Difficulties in long-term follow-up: tracing subjects during long periods of time is difficult and results in biases due to loss to follow-up; collecting information on incident diseases may also be problematic.
- Access to different sources of data: the follow-up usually implies frequent contacts with the subjects, plus the linkage to various data bases; this may pose legal problems regarding data privacy, and requires important technical skills.
- Long term implication: the most fruitful cohorts expend over decades and it is difficult to guaranty the stability of the scientific and technical staff, as well as permanent funding.
- High cost: depending of the size of the cohort and of the nature and quantity of individual data collected, budgets may largely vary, but are always important. A recent official report showed that in France the annual cost per subject of epidemiological longitudinal cohorts is currently comprised between 25 Euros (about32.5US dollars) and 250 Euros (about325US dollars). One of the main determinants of differences was the availability of already existing data which partly avoid the cost of data collection [Valleron, 2005].
Facing these difficulties, it would be too costly that each research group sets up its own cohort for its specific needs, and it seems important to consider that the design and organization of longitudinal epidemiological cohorts should favor two main aspects:
- General-purpose design: in order to be able to look at various epidemiological questions, the samples should be diversified in terms of demographic and social characteristics, and the collection of individual data should be comprehensive in terms of determinants and health conditions; supplementary data maybe collected when necessary, allowing for in depth analysis of specific problems.
- Open access data set: access to the cohorts‘subjects and data should be largely open and shared by the research community, allowing for substantial savings in efforts and budgets.
Finally, epidemiological cohorts should be constructed as —open general-purpose longitudinal epidemiological laboratories“. That is what we have tried to do in our group, first with the GAZEL cohort, and currently through the CONSTANCES project.
References
Goldberg M, Chastang JF, Leclerc A, Zins M, BonenfantS, Bugel I, Kaniewski N, Schmaus A, Niedhammer I, Picio i M, Chevalier A, Godard C, Imbernon E. Socioeconomic, demographic, occupational and health factors associated with participation in a long-term epidemiologic survey. A prospective study of the French gazel cohortand its targetpopulation. Am JEpidemiol 2001; 154:373-384.
Melchior M, Goldberg M, Krieger N, Kawachi I, Menvielle G, Zins M, Berkman LF Occupational class, occupational mobilityand cancer incidence among middle-aged men and women: a prospective studyof the French GAZELcohort. Cancer Causes Control. 2005;16:515-24.
Menvielle G, Luce D, Geoffroy-PerezB, Chastang JF, Leclerc A. Social inequalities and cancer mortalityin France, 1975-1990. Cancer Causes Control. 2005; 16:501-513. Szklo M. Population-based cohortstudies. Epidemiologic Reviews 1998;20: 81-90.
Valleron AJ(Ed). L‘épidémiologie humaine en France. Rapportscientifique ettechnique. Paris, Académie des Sciences, 2005.
2. The GAZEL Cohort1
2.1. Objectives
The GAZEL cohort was launched in January1989. Designed as a research tool, it was intended to facilitate epidemiological research on various diseases and multiple health-related factors. Because it was not designed to study a specific issue, the GAZEL cohort constitutes an open and general-purpose epidemiological laboratory. The project relies on a long-term follow-up of the cohort, which includes the systematic and prospective collection of various data from different sources. These data are available to investigators conducting research projects within the cohort. In addition, the cohort offers an easy access to a large group of volunteers willing to participate in epidemiological research, allowing for the collection of additional data.
Any research group, in France or elsewhere, can submit a research proposal involving the GAZEL cohort. These projects are reviewed by a Scientific Committee, and those selected receive free access to the GAZEL data and subjects.
2.2. Setting
The GAZEL cohort is composed of workers at Électricité de France-Gaz de France (EDF-GDF), the only utility company in France. For several reasons, EDF-GDF is a unique setting for a long-term general purpose epidemiological cohort.
- A large and diversified population: EDF-GDF employs workers in all regions of France, from large cities to small villages. There is a wide socioeconomic range of occupational positions, including white and blue-collars workers.
- The workforce is very stable: due to their civil servant-like status, employees almost never leave the company and are not lost to follow-up even after retirement, since retirement benefits are paid by the company itself. An extensive, efficient human resources file system allows for a complete follow-up of the cohort workers, even when they move or retire.
- EDF-GDF has its own occupational health and social security system: about 300 physicians work for the company and are responsible for health surveillance among the workers; specific information systems systematically register data on the health problems and working conditions of the workforce.
2.3. Main characteristics of the cohort
At baseline, the GAZEL cohort comprised 20,625 individuals: 15,011 men aged from 40 to 50 years in January 1989(mean: 45years), and 5,614 women aged from 35 to 50 years at that time (mean: 42 years). The number and percentage of participants belonging to the main occupational groups is reported in the following table. 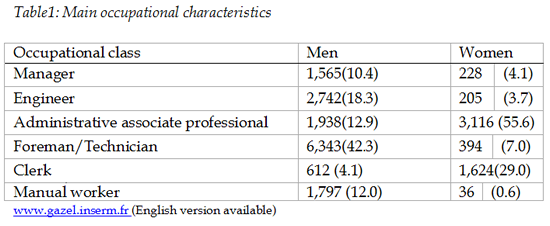
2.3.1. Data
Since 1989, INSERM Unit 687 has systematically collected data from different sources. These data are made available to investigators after their research project has been submitted and accepted by the GAZEL Scientific committee.
Each year a self-administered questionnaire is sent to each participant at home. Data on health, lifestyle, individual, familial, social and occupational factors and life events are collected through these questionnaires.
Some of the data collected are intended to reflect psychosocial factors. Each year, subjects answer questions about their main life events and the social support they receive. Detailed data on social networks has been recorded. The French versions of the Job-strain questionnaire and the Effort reward-imbalance questionnaire were also regularly completed. Data on working conditions and tasks performed bythe workers come from the occupational physicians and the subjects themselves. The database also contains various mental health scales, completed atdifferentpoints of follow-up.
Various sources within EDF-GDF provide additional data about GAZEL participants. Occupational and personal data are updated through human resources department files. Medical data on sick leaves and incidence of cancer and coronary heart diseases come from the company’s Health Insurance Department. Occupational physicians collect data on working conditions, occupational exposures to chemicals trough MATEX (a job-exposure matrix specific of the company), and the physical examination of the workers.
Sources outside EDF-GDF also provide data -on causes of death, health care use, and hospitalizations. Every five years, volunteers are invited to visit a health screening center run by the National health insurance fund, where they undergo a full standardized medical examination that includes the collection of blood samples.
The following table summarizes the different types of data collected systematically and routinely from different sources for each participant in the GAZEL cohort.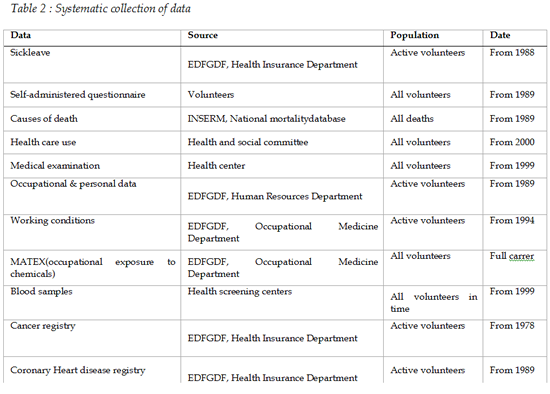
2.4. Follow-up
As they have aged, about75% of the workers of the cohort have retired by the end of 2004(men: 87%; women: 62%) and 901 died (men: 764; women: 137).
The GAZEL cohort is characterized by a very low loss to follow-up. Members of the cohort are followed and data are collected from medical and non-medical sources even if they do not complete their annual self-administered questionnaire. During the first16 years of follow-up (1989-2004), only126 subjects (0.6%) were lost to follow-up (six participants decided to quit the cohort, 120 had left the company during that period).
The annual response rate to the self-administered questionnaire is also an important indicator of the quality of follow-up. After a fall during the first 5 years of follow-up, almost75% of the questionnaires are now returned every year. As it is not always the same persons who fail to respond each year, fewer than 3% of the initial cohort have never sent back their questionnaire.
This high participation rate is a very important feature for researchers who develop specific projects for the GAZEL cohort: despite the wide range of data systematically collected, a specific research project often requires the collection of additional data. Accordingly, investigators have access not only to the database, which is maintained by the INSERM Unit 687, but they can also contact the volunteers directly with supplementary questionnaires or specific examinations. They also benefit from the systematic follow-up of the cohort and can link their own data to the health events recorded in the database.
2.5. Research within the GAZEL cohort
The GAZEL data base is freely open for the selected research projects, but when extra costs are involved for specific research projects, they have to be supported by the investigators.
Almost 30 research projects conducted by more than 15 groups from different countries (France, UK, Germany, Belgium, USA, Canada) are currently ongoing within the cohort. These projects are focused on various physical and mental health conditions and on many different determinants, especially occupational factors. The titles of the currently ongoing research projects are listed in the Appendix, as well as selected references.
As the cohort is ageing (mean age in 2005: 62and 59for men and women respectively), and as most of the subjects are retired, new research projects are more and more focusing on various determinants of health in early old age, taking advantage of the large amount of data prospectively collected from baseline, when subjects were middle-aged (men: from 40 to 50 years; women from 35 to 50 at baseline). This almost unique feature of GAZEL allows studying determinants of various physical and functional aspects of ageing earlier in life than in most of the ageing cohorts.
2.5.1. Funding
GAZEL is a “low cost“cohort (annual cost per participant: 25 Euros, i.e. about 32.5 US dollars), thanks to the numerous data provided by the company. A large part of the funding of GAZEL came from EDF-GDF, the company being interested in the health of its workforce. However, the vast majority of the cohort participants being now retired, EDF-GDF has decided to stop its financial participation to the project after 2006. Seeking support from research grants is the usual way for projects addressing specific research questions. It is however much more difficult to find regular resources for routine data collection and management, which is nevertheless absolutely necessary for developing specific projects within the cohort.
3. The CONSTACES Project
While GAZEL proved to be a very efficient research tool, yielding numerous findings in various epidemiological fields and giving new opportunities for studying ageing, the cohort has some limits as a general-purpose longitudinal epidemiological laboratory. They are mainly due to its limited size, the restricted age range, and the specific social and occupational characteristics of the EDF-GDF population. This is why, taking advantage of the experience of GAZEL, we launched the CONSTANCES project.
CONSTANCES is also a longitudinal cohort designed as a general-purpose epidemiological laboratory, open to the international research community. Compared to GAZEL, it will be much larger in size, general population-based, and including a wider range of age classes. The cohort will be a research tool, intended to facilitate epidemiological research on various outcomes and health-related factors. More specifically, CONSTANCES will be a research toll to examine social determinants of health and health inequalities, with a focus on ageing, employment and working conditions.
3.1. Setting
CONSTANCES takes place within the “Régime general” of the French Social security system. The population covers employees of the private sector and their family (self-employed persons and agricultural workers are excluded); 80% of the French population (about 50 million) is affiliated to the “Régime general”, and everyone is entitled to a free health screening every 5 years. For this purpose, about 100 Health screening centers (HSC) were established in all regions of France, and about 650,000 individuals visit a HSC each year. The participants of CONSTANCES will be recruited among them on a voluntary basis.
3.2. Design of the cohort
3.2.1. Structure
The sample at inception will be proportional to the structure of the general population covered by the “Régime general” for age (18-70 years range), gender and SES; it size will be at least 200,000 subjects, included over a 5 years period, starting at the end of 2006. Participants will be recruited in 16 HSCs from different regions of France (see map below). 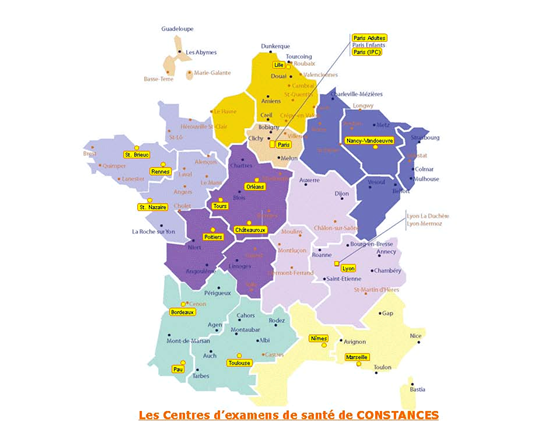
3.2.2. Inclusion
The inclusion of the full cohort will extend over 5 years (about 50,000 subjects every year).
Subjects will receive a letter invitation to come to the HSC (including a self-administered questionnaire), and undergo a health screening. Data collected directly from the participants through questionnaires and from the medical screening will mainly include:
- socioeconomic status (SES) data: current SES (professional condition, education level, income and wealth, subjective SES, spouse SES, material conditions such as housing and equipment, financial support, neighborhood), SES history(social and geographical origin, main life events, job history);
- social network: family, work, neighborhood, social and leisure activities;
- occupational data: job history, occupational exposure (history and current: organizational and ergonomic factors, chemicals and biological exposure, psychosocial factors); a job-exposure matrix specific of the French population will also be used to link occupational histories with occupational exposure to chemicals;
- lifestyle data: drinking, smoking, physical activities, eating habits, leisure activities;
- health data: personal and familial medical history, various mental and somatic health scales, physical and biological screening (biometry, blood pressure, respiratory function, vision and audition, dental health, current diseases, main blood parameters, DNA samples)
A focus will be put on topics of special interest: women (specific health and SES questionnaire), and ageing (specific health and SES questionnaire, specific health screening using a battery of cognition and physical functioning tests). Standardized procedures for data collection and quality control are currently under development. They include also the regular training of the personal of the HSC and frequentsite visits.
3.2.3. Follow-up
The follow-up of the cohort members will rely on two different types of procedures:
- Active follow-up procedure will include annual mail questionnaires (occupational status, working conditions and exposures, housing, life habits, life events, health scales and disease incidence and treatment, social network…), and regular visits to the HSC.
- Passive follow-up procedures will include regular linkage to national data bases: morality data base (vital status, cause of death), retirement fund data base (occupational status, plus postal address), health data bases (doctor‘s visits, hospitalization, treatments, …).
A technical platform for handling and recording questionnaires, extracting data for individual cohort participants from national health and retirement fund data bases trough highly secured procedures and managing the cohort data base is currently being established.
A number of different procedures will be implemented for tracing subjects: linkage to social security and retirement fund data bases, tracing of postal addresses through the national postal service.
Strategies for minimizing non-response during follow-up will benefit from the experience developed for GAZEL. Each year all participants will receive, with the new questionnaire and return envelope, a letter from the principal investigator and an issue of a newsletter, which informs them of studies currently underway, scientific publications, and the new side-studies in preparation. It will also include a "letters" column, printing the most typical of the letters received. Three months later, a reminder will be send to those who did not respond to the first mailing. A scientific symposium will also be organized each year and a web site is currently under development. Finally, we will publicize CONSTANCES in the medical press and the general media, in order to reinforce its credibility for cohort members.
3.2.4. Organization
A project team was established (“Cohort team“of the INSERM-CNAMTS Research Unit), as well as a project group to help with the protocol (more than 20 epidemiologists from various specialized groups: Inserm, University, InVS…), and an operational group including the HSCs. An intranet specific to the project is being developed. All procedures for inviting the subjects, organizing their stay in the HSC, collecting data from the different sources, controlling the quality of data, monitoring the flows of participants and of data, storing and transmitting the data are currently under development.
An international Scientific Comittee is already established. A call for research proposals will be launched in the second part of 2006, asking research groups to apply for research projects within the cohort. The Scientific Committee will also actas a selection body.
3.2.5. Legal aspects
Complex procedures are currently defined to ensure the confidentiality of the CONSTANCES data base and the linkage to national data bases for extracting personal data for the participants. They mainly rely on the physical separation between the files containing nominative data and the files recording personal data, the utilization of algorithms for data encrypting and the use of different anonymous identification numbers for the linkage with national data bases. These procedures are currently under development in collaboration with the officials of the “Commission Informatique et Libertés“, the French legal authority for data privacy.
3.2.6. Timetable
- Scientific protocol finalized: December 2005.
- Operational protocol finalized (including legal authorizations): June 2006.
- Pilots: December 2005œ May2006 (including real inclusion of the participants).
- Firstfull inclusions: January2007.
3.2.7. Funding
The funding of the CONSTANCES project comes mainly from the Social security-CNAMTS. The estimation of the total annual cost is about 2 millions Euros (2.6 millions US dollars) for the whole cohort (approximately 10 Euros/subject, i.e. 13 US dollars). This low cost is due to the fact that CONSTANCES heavily relies on existing structures (HSCs, health and retirement fund data bases) with only small extra costs.
However, the budget currently does not include specific funding for the biobank. One of major problem is the large storage facilities needed to accommodate huge numbers of biological samples, and discussions are currently under way with the French ministry of research.
The funding will cover the routine operations for the regular functioning of the cohort. As for GAZEL, the data base will be freely open for the selected research projects, but any extra costs involved for specific research projects will have to be supported by the investigators.
3.3. Appendix
3.3.1. Current research projects within GAZEL
- Determinants of Ageing: Whitehall II – GAZEL Comparative Analyses *
- Predictors of Cognitive Function in Early Old Age: Whitehall II -GAZELComparative Analyses *
- Social Productivity and Health in Early Old Age *
- Work Absenteeism for Anxiety and/or Depression and Ischemic Heart Disease
- Evolution of Musculoskeletal Disorders and Long-Term Effects of Occupational Exposure
- Absenteeism Research Methodology: an Evaluation and a New Perspective
- Use of Cellular Telephones and Migraine*
- Occupational Exposure to Chemicals and Cognitive Function after the age of 55
- Working Conditions and Long-Term Incidence of Musculoskeletal Diseases*
- Social Determinants of Mental Health
- Sociospatial Disparities in Health Status
- Psychosocial Factors and Social Inequalities of Cardiovascular Health
- Psychosocial Factors at Work and Health in the GAZEL Cohort
- Determinants of Consumption of Alcoholic Beverages
- Epidemiologyof Cancer in the GAZEL Cohort
- The Influence of Social Networks and Suppor ton Cardiovascular Health *
- Periarticular Rheumatological Conditions and Work Motions *
- Course and Consequences of Migraine *
- Occupational Risk Factors for Low Back Pain among Groups of EDF-GDF Workers *
- Sleep Hygiene, Somnolence and Quality of Life *
- Insomnia and Evolution of the Incidence of Psychiatric Pathologies *
- Epidemiology of Traffic Accidents *
- Depressive Disorders in the GAZEL Cohort *
- Chronic Disease: its Repercussions on Occupation and Family
- Psychological Factors Predictive of Ischemic Heart Disease and Cancer
- Menopause and Osteoporosis *
- Urinary Incontinence and Menopause: Risk Factors and Quality of Life *
* Projects including the collection of supplementary data
3.3.2.Selected publications from GAZEL
Ringa V., Ledesert B., Breart G. Determinants of hormone replacement therapy among postmenopausal women enrolled in the French GAZEL cohort. Osteoporosis International, 1994, 4, 16-20.
Boumendil E. Descriptive study of lipid modulating drug use in a French professional population. Journal of Clinical Epidemiology, 1994, 47, 10, 1163-1171.
Ledesert B., Ringa V., Breart G. Menopause and perceived health status among the women of the french GAZEL Cohort. Maturitas, 1995, 20, 113-120.
Boumendil E., Tubert-Bitter P. Depression-induced absenteeism in relation with antihyperlipidemic treatment: a study using GAZEL Cohort data. Epidemiology, 1995, 6, 3, 322-325.
Moneta G., Leclerc A., Chastang J.F., Dang Tran P., Goldberg M. Time-trend of sleep disorder in relation to night work: a study of sequential one-year prevalences within the GAZEL Cohort. Journal of Clinical Epidemiology, 1996, 49, 10, 1133-1141.
Michel P., Dartigue J.F., Lindoulsi A., HenryP. Loss of productivity and quality of life in migraine sufferers among French workers: results from the GAZEL Cohort. Headache, 1997, 37, 71-78.
Niedhammer I., Goldberg M., Leclerc A., David S., Bugel I., Landre M.F. Psychosocial work environment and cardiovascular risk factors in an occupational cohort in France. Journal of Epidemiology and Community Health, 1998, 52, 93-100.
Dartigues J.F., Michel P., Lindoulsi A., Dubroca B., Henry P. Comparative view of the socioeconomic impact of migraine versus low back pain. Cephalalgia, 1998, suppl 21, 26-29.
Niedhammer I., Bugel I., Goldberg M., Leclerc A., Gueguen A. Psychosocial factors at work and sickness absence in the GAZEL cohort: a prospective study. Occupational and Environmental Medicine, 1998, 55, 735-741.
Dang Tran P., Leclerc A., Chastang J.F., Goldberg M. Regional disparities in cardiovascular risk factors in France : A five-year analysis of the GAZEL Cohort. European Journal of Epidemiology, 1998, 14, 535-543.
Niedhammer I., Goldberg M., Leclerc A., Bugel I., David S. Psychosocial factors at work and subsequent depressive symptoms in the GAZEL cohort. Scandinavian Journal of Work, Environmentand Health, 1998, 24, 3, 197-205.
Niedhammer I., Goldberg M., Leclerc A., David S., Bugel I., Landre M.F. Facteurs psychosociaux au travail : utilisation du modèle de Karasek et application à l‘étude des facteurs de risque cardio-vasculaires dans la Cohorte GAZEL. Revue de Médecine du Travail, 1998, 25, 28.
Boumendil E.F., Mugnier C. Antihypertensive drug treatment and of the population treated. American Journal of Hypertension, 1998, 11, 929-934.
Zins M., Carle F., Bugel I., Leclerc A., Di Orio F., Goldberg M. Predictors of change in alcohol consumption among Frenchmen of the GAZEL study cohort. Addiction, 1999, 94, 3, 385-395.
Niedhammer I., Bugel I., Bonenfant S., Goldberg M., Leclerc A. Validity of self-reported weight and height in the French GAZEL Cohort. International Journal of Obesity, 2000, 24, 1111-1118.
Fauconnier A., Ringa V., Delanoë D., Falissard B., Breart, G. Use of hormone replacementtherapy: women‘s representations of menopause and beauty care practices. Maturitas, 2000, 35, 215-228.
Goldberg P., Gueguen A., Schmaus A., Nakache J.P., Goldberg M. Longitudinal study of associations between perceived health status and self-reported diseases in the French GAZEL cohort. Journal of Epidemiology and Community Health, 2001, 55, 233-238.
Taillard J., Philip P., Chastang J.F., Diefenbach K., Bioulac B. Is self-reported morbidity related to the circadian clock? Journal of Biological rhythms, 2001, 16, 2, 183-190.
Goldberg M., Chastang J.F., Leclerc A., Zins M., Bonenfant S., Bugel I., Kaniewski N., Schmaus A., Niedhammer I., Piciotti M., Chevalier A., Godard C., Imbernon E. Socioeconomic, demographic, occupational and health factors associated with participation in a long-term epidemiologic survey. A prospective study of the French GAZEL Cohort and its target population. American Journal of Epidemiology, 2001, 154, 4, 373-384.
Philip P., Taillard J., Niedhammer I., Guilleminault C., Bioulac B. Is there a link between subjective daytime somnolence and sickness absenteeism? A study in a working population. Journal of Sleep Research, 2001, 10, 2, 111-115.
Ribet C., Lang T., Zins M., Bingham A., Ferrieres J., Arveiler D., Amouyel P., BonenfantS., Chastang J.F., Goldberg M., Ducimetiere P. Do cardiovascular risk factors in men depend on their spouses‘ occupational category? European Journal of Epidemiology, 2001, 17, 347-356.
Metzger M.H., Goldberg M., Chastang J.F., Leclerc A., Zins M. Factors associated with self-reporting of chronic health problems in the French GAZEL Cohort. Journal of Clinical Epidemiology, 2002, 55, 48-59.
Niedhammer I. Psychometric properties of the French version of the Karasek Job Content Questionnaire: a study of the scales of decision latitude, psychological demands, social support, and physical demands in the GAZEL Cohort. International Archives of Occupational and Environmental Health, 2002, 75, 3, 129-144.
Tubach F., Leclerc A., Landre M.F., Pietri-Taleb F. Risk factors for sickness absence due to law back pain: a prospective study. Journal of Occupational and Environmental Medicine, 2002, 44, 5, 451-458.
Furher R., ShipleyM.J., Chastang J.F., Schmaus A., Niedhammer I., Stansfeld S.A., Goldberg M., Marmot M.G. Socioeconomic position, health, and possible explanations: a tale of two cohorts. American Journal of Public Health, 2002, 92, 8, 1290-1294.
Paterniti S, Niedhammer I, Lang T, Consoli Sm. Psychosocial factors at work, personality traits and depressive symptoms. British Journal of Psychiatry, 2002, 181, 111-117.
Melchior M, Berkman L, Niedhammer I, Chea M, Goldberg M. Social relations and self-reported health: a prospective analysis of the French GAZEL Cohort. Social Science and Medicine, 2003, 56, 1817-1830.
Melchior M, Niedhammer I, Berkman Lf, Goldberg M. Do psychosocial work factors and social relations exert independent effects on sickness absence? A six-year prospective study of the GAZEL cohort. Journal of Epidemiology and Community Health, 2003, 57, 4, 285-293.
Leclerc A, Tubach F, Landre Mf, Ozguler A. Personal and occupational predictors of sciatica in the GAZEL cohort. Occupational Medicine, 2003, 53, 6, 384-391.
Niedhammer I, Chea M. Psychosocial factors at work and self-reported health: comparative results of cross-sectional and prospective analyses of the French GAZEL Cohort. Occupational and Environmental Medicine, 2003, 60, 509-515.
RibetC, Zins M, Bingham A, Goldberg M, Ducimetiere P, Lang T. Occupational mobility and risk factors in working men: selection, causality or both? Results from the GAZEL study. Journal of Epidemiology and Community Health, 2003, 57, 11, 901-906.
Allonier C, Chevalier A, Zins M, Catelinois O, Consoli S, Goldberg M, Lahon G. Anxiety or depressive disorders and risk of ischemic heart disease among French power company employees. International Journal of Epidemiology, 2004, 33:1-8.
Berkman L.F., Melchior M., Chastang Jf., Niedhammer I., Leclerc A., Goldberg M. Social integration and mortality: a prospective study of French men and women employees of Electricity of France-Gas de France, the GAZEL Cohort. American Journal of Epidemiology, Am J Epidemiol, 2004; 159: 167-174.
Lagarde E, Chiron M, Lafont S. Traffic ticket fixing and driving behaviours in a large French working population. J Epidemiol Community Health. 2004; 58:562-8.
Lagarde E, Chastang JF, Gueguen A, Coeuret-Pellicer M, Chiron M, Lafont S. Emotional stress and traffic accidents: the impact of separation and divorce. Epidemiology. 2004; 15:762-6.
Niedhammer I, Tek ML, Starke D, Siegrist J. Effort-reward imbalance model and self-reported health: cross-sectional and prospective findings from the GAZEL cohort. Soc Sci Med. 2004:1531-41.
Ringa V, Varnoux N, Piault S, Breart G. Hormone therapy use among postmenopausal French women before the publication of the Women's Health Initiative study: duration of use and factors associated with discontinuation. Fertil Steril. 2005, 83:1771-9.
Melchior M, Krieger N, Kawachi I, Berkman Lf, Niedhammer I, Goldberg M. Work Factors and Occupational Class Disparities in Sickness Absence: Findings From the GAZEL Cohort Study. Am J Public Health 2005, 95: 1206-1212.
Melchior M, Goldberg M, Krieger N, Kawachi I, Menvielle G, Zins M, Berkman LF. Occupational class, occupational mobility and cancer incidence among middle-aged men and women: a prospective study of the French GAZEL cohort. Cancer Causes and Control 2005, 16: 515œ524.
Lagarde E., Chastang Jf., LafontS., Coeuret-Pellicer M., Chiron M. Pain and pain treatment were associated with traffic accident involvement in a cohort of middle-aged workers. Journal of Clinical Epidemiology, 2005, 58: 524-531.
Sanchez-Ortuno M., Moore N., Taillard J., Valta C., Leger D., Bioulac B., Philip P. Sleep duration and caffeine consumption in a French middle-aged working population. Sleep Medicine, 2005, 6: 247-25.
Nabi H., Consoli Sm., Chastang Jf., Chiron M., Lafont S., Lagarde E. Type A Behavior Pattern, Risky Driving Behaviors, and Serious Road Traffic Accidents: A Prospective Study of the GAZEL Cohort. American Journal of Epidemiology, 2005, 161: 864-870.
Nachit-Ouinekh F., Chrysostome V., HenryP., Sourgen C., Dartigues J.F., El Hasnaoui A. Variability of reported headache symptoms and diagnosis of migraine at12months. Cephalalgia, 2005, 25: 117-123.
Galera C., Fombonne E., Chastang J.F., Bouvard M.P. Childhood hyperactivity-inattention symptoms and smoking in adolescence. Drug and Alcohol Dependence, 2005, 78: 101-108.
Parmentier G, Chastang JF, Nabi H, Chiron M, Lafont S, Lagarde E. Road mobility and the risk of road traffic accident as a driver. The impact of medical conditions and life events. Accid Anal Prev, 2005,37:1121-34.
 Click on the PFD icon above to download the entire paper
Click on the PFD icon above to download the entire paper