


A Survey of Health, Ageing and Retirement in Europe
Arie Kapteyn
Senior Economist
1. Introduction
The Survey of Health, Ageing, and Retirement in Europe (SHARE) is patterned after the Health and Retirement Study in the U.S. and interviews respondents over 50 in a number of European countries. It is a young survey. In the fall of 2004, a first wave was conducted in eleven European countries (Germany, Switzerland, Belgium, Greece, Netherlands, Italy, Austria, Sweden, Denmark, France, Spain) covering about 18,000 households and 27,000 respondents. Most of the funding has come from the European Union, with additional funding in some countries from national sources. A strategically very important source of funding has been the National Institute on Aging in the United States. A second wave is foreseen in the fall of 2006. The number of countries will expand by at least four: Israel, Czech Republic, Poland, and Ireland. The survey for Israel is currently in the field. Despite its short history, SHARE has built considerable momentum, which is ground for optimism regarding both future funding and the number of countries participating. In this paper we provide a brief sketch of the history of SHARE, its funding sources, the organization and its scientific aims. We devote some space to thoughts why SHARE appears to be successful and end with some speculations on what the future directions of SHARE may be.
2. Brief History and Organization
Strictly speaking the history of SHARE starts with the U.S. Health and Retirement Study, which has proved to be a powerful model for modern large-scale data collection projects for scientific purposes. Various related efforts have sprung up in different countries, including the English Longitudinal Survey of Aging (ELSA, http://www.ifs.org.uk/elsa/) and the Mexican Health and Aging Study (MHAS, http://www.mhas.pop.upenn.edu/).
The initiative for SHARE primarily came from a number of U.S. researchers involved in HRS, and from NIA. A very early discussion about setting up a European HRS took place during an international conference on aging in Amsterdam in the summer of 1997. As an outgrowth of that Jim Smith (RAND) and Richard Burkhauser (Cornell) organized a meeting at the Rockefeller Bellagio Study and Conference Center in July 1999. In parallel, NIA sponsored an NRC panel on "Preparing for an Aging World; the Case for Cross-National Research" (NRC, 2001). The report of the panel made a strong case for the importance of international comparative research and how comparable data are needed for that.
At the Bellagio meeting it was agreed "to explore the feasibility of a European Health and Retirement Survey, and to begin to lay the foundation for undertaking such a survey". Arie Kapteyn was designated as a potential PI for the European HRS. At the suggestion of Richard Suzman he drafted an Interagency Agreement (IAG) that was concluded subsequently between NIA and the United Nations ECE program in Geneva. The citation above is actually from this IAG. The IAG was partly used to support a planning conference in Venice, Italy in February 2002.
During 2000 Arie Kapteyn accepted a position at RAND in Santa Monica, California, so that a new PI had to be found. At a TMR meeting in Paris in October 2000 a core group of researchers consisting of Agar Brugiavini, Tito Boeri, Axel Boersch-Supan, Michael Hurd, Arie Kapteyn, Marie-Louise Kemperman, Jim Smith, and Bob Willis came together to discuss the possibility of launching a European variant of HRS and who could lead such an effort. Due consideration was given to an initial choice of countries, where good groups of researchers were expected to be willing and able to help in the endeavor. In view of the background of the researchers it was not surprising that a strong overlap existed between the initially selected countries and the countries participating in the TMR network. Axel Boersch-Supan was asked to be PI. The core group initially consisted exclusively of economists, so a first priority has been to expand the number of disciplines. Although economists still form a major part of the total group of researchers involved, disciplines now include epidemiologists, sociologists, psychologists, psychiatrists, and statisticians.
At the IAG financed conference in Venice it was decided to apply for funding from the European Commission under its fifth framework program. The framework programs are essentially five-year research funding programs. Finding the right umbrella under which a research project may fall is always a bit of an effort and redefining research ideas so that they fit bureaucratic rules has become somewhat of an art. The various funding programs all have limits on the size of awards and it was clear from the start that a Europe-wide SHARE would simply be too expensive to fit under any existing umbrella. Thus the funding of SHARE had to be put together from a number of smaller funding sources, as is described in more detail in the next section.
The first grants were obtained from the EU during 2002, while in addition NIA provided support to the Survey Research Center of the University of Michigan to provide technical assistance. Furthermore a second IAG provided support for experiments, as explained more fully in Section 3. After a preparatory period of about a year and a half the first wave of data was collected in 2004.
SHARE wave 1 data were collected in May October 2004. A very preliminary version of the data was released on November 15, 2004. In April 2005, "Release 1" was made available to the scientific community at large. This has still a preliminary nature, but has undergone some cleaning, has constructed harmonized variables like education level, personal income, household wealth, and has sampling weights correcting for stratified sampling and unit non-response. Table 9.1, taken from De Luca and Peracchi (2005) provides an overview of sample sizes and response rates. SHARE response rates compare fairly favorable to response rates of other European surveys, although they are lower than response rates typically found in North America.
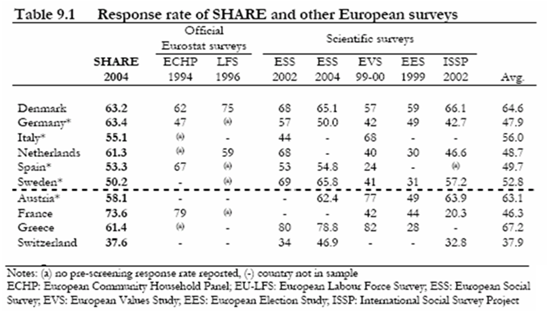
Table 9.11 also taken from De Luca and Peracchi (2005) shows the sample sizes of the so-called core sample in the various countries; these numbers do not include the additional vignette samples drawn in a number of countries (see below).

The data can already be used to illustrate many interesting issues, relating to the unique multi-disciplinary and multi-country nature of SHARE. Here we provide a few examples. The complete first result book can found at: http://www.share-project.org/. Recently a second book mainly devoted to methodological issues came out. This is also available on the Web.
2.1. The oldest old
16% of all oldest old (80+) live with their family, most often with a child. This is very unevenly distributed across SHARE countries, however, with the highest proportions in Italy (22%) and Spain (37%). This may reflect cross-national differences in institutions such as access to nursing homes, or cross-cultural differences in caring for family members. A challenging finding in this respect is that, when asked who should care for the elderly, respondents in northern Europe typically think this is a task for the government, while respondents in Southern Europe tend to mention the family. About 22% of the oldest old are socially active. There is substantial cross-country variation in the nature of the activities. For example, more than 40% of the oldest old in Greece are active in a religious organization, versus less than 10% for SHARE as a whole. On the other hand, Denmark and the Netherlands have the highest participation rates in sports clubs and social clubs (21% and 19% versus an average of 7%). While cross-country comparisons in mortality and life expectancy do not show a clear pattern, SHARE shows an intriguing north-south gradient in various health and economic outcomes for the oldest old. Oldest old in the north are healthier and have higher (PPP-adjusted) income.
2.2. Housing
Housing and living arrangements are central aspects of the welfare position of the elderly. The transition to retirement greatly increases the importance of one's home. The 50+ in Europe have typically lived in the same home for a long time. For the 50-59 age group, the average in their current dwelling is between 14 years (Sweden) and 22 years (Italy and Austria). For the older age groups, there is a clear north south gradient in this respect, with an average time spent in the current dwelling of more 20-25 years in the Scandinavian countries and the Netherlands, versus more than 30 years in Austria, Greece, Spain and Italy.
Home ownership rates in SHARE range from 53% in Germany to 87% in Spain. The large cross-country differences create an excellent opportunity to study the effect of variations in institutions. The SHARE countries vary enormously in the way in which home ownership is taxed, in tax deduction opportunities of mortgage payments, and in subsidized renting. For example, the high rate of tenants in the Netherlands is mainly a cohort effect, due to the historically large regulated and subsidized social segment of the rental market with low-income households paying artificially low rents. In most countries the higher income groups have more home-owners, but in the Netherlands the SES-gradient is particularly steep.
2.3. Physical Health, Health Behavior and Obesity
It is well known that self-reported health measures suggest substantial differences in the distributions of health across countries, and SHARE is no exception to this. For example, Germans tend to rate their health more negatively than the Dutch or Danes. Perhaps more surprisingly, SHARE also shows substantial differences across countries in objective measures such as grip strength and walking speed. Both go in the same direction: there is a clear north-south gradient within Europe, with higher prevalence of low grip strength and low walking speed in the south, particularly in Spain and Italy.
Results from SHARE are consistent with an extensive body of research showing large socio-economic disparities in physical health across Europe. This also applies to objective measures like grip strength and walking speed, for both men and women. On average, respondents with low education are 30% more likely to be in the lowest grip strength quartile than the higher educated, and a similar relation is found between grip strength and income. These relationships appear to be quite strong in each of the SHARE countries.
The same gradient is also apparent in physical activity and obesity. On average, the low educated are 70% more likely to be physically inactive, controlling for country, age, and gender. A similar gradient is found for smoking behavior, but not for drinking alcohol. If anything, the higher educated drink more than the lower educated. The low educated have a 25% higher probability to be overweight (body mass index (BMI) larger than 25) and a more than 50% higher probability to be obese (BMI>30). Obesity and overweight seem to have become a serious health threat among the 50+ populations in the SHARE countries, although prevalence is lower than in the US. Of the birth cohort 1931-1950, obesity rates among men in the SHARE countries vary from 14% in the Netherlands to 21% in Spain, compared to about 30% in the US (see Michaud and Van Soest, 2005). For women, the SHARE rates vary from 14% in Denmark to 28% in Spain, compared to 30% for the US. The negative relation between income and obesity is quite salient in all countries.
2.4. Mental Health
Major depression is forecast by 2020 to have risen from the fourth to the second most burdensome health condition worldwide, taking into account both associated disability and premature mortality (Murray and Lopez, 1997). The SHARE survey includes the EURO-D scale, validated in an earlier cross-European study (Prince et al., 1999a,b). Those with a EURO-D score exceeding 3 are considered likely to be diagnosed as suffering from a depressive disorder. Prevalence of current depression rises with age in most SHARE countries and is higher among women than among men. Particularly the southern European countries show a large gender gap with huge depression prevalence rates among elderly women. Both past and current depression is significantly larger among unmarried respondents than among married respondents.
Interestingly, there is a clear negative association between depression and income or wealth in the northern countries, but such an association is completely absent in the south of Europe (controlling for age, sex and marital status). Whether this is related to differences in institutions, family networks, etc., is worth investigating. Longitudinal data will be useful to identify the causal chains of events.
2.5. Cognitive Impairment
Cognitive ability in SHARE was measured in several dimensions: memory recall, verbal fluency, and numeracy. However measured, cognitive ability is strongly associated with education the higher educated are more cognitively able than the lower educated. Cross-country differences between cognitive impairment rates seem quite well in line with cross-country differences in education level. For numeracy, the relation with education is much stronger in the southern countries than in, particularly, Denmark and Sweden. In the latter countries, we find the strongest positive association between cognitive ability and wealth or income.
2.6. Health Care
Health insurance arrangements vary enormously across the SHARE countries, providing an ideal setting for studying the consequences of institutional variation across countries. Many countries have a general public health insurance system, financed either through national, regional or local taxes, or through social contributions depending on income level. Similar to the US, Switzerland has a private health care system, but it is compulsory for everyone. In Germany, 9% are not covered by the public health care system (mainly civil servants) and have private compulsory health insurance. In the Netherlands, the higher income groups (25%) have non-compulsory private insurance. However, since 2006, everybody has the obligation to have a private insurance, which may be (partly) reimbursed for low-income groups. In the other countries, private insurance often covers supplemental health care. In France, 85% have some supplemental insurance, compared to 10% in Spain and Greece.
Differences in out-of-pocket medical expenditures illustrate the cross-country differences in health care systems. In Germany, Sweden, Denmark and Greece, more than 80% of SHARE households have at least some out-of-pocket expenditure in the past 12 months. In France, Spain, and the Netherlands, the percentages are only 37%, 41% and 42%, respectively. There are significant differences in out of pocket expenditures (both prevalence and mean) of respondents with and without supplemental health insurance, but the difference is sometimes positive and sometimes negative, perhaps related to the institutional nature of the supplemental insurance. In Italy and Austria, for example, households with supplemental insurance have a significantly higher probability of having out of pocket expenditures than others, and also spend significantly more. This could suggest that those with supplemental insurance are those with higher demand for health care. In Greece, on the other hand, households with supplemental insurance are less likely to have out of pocket expenditures than those without. These differences suggest that a careful study of the relation between differences in the insurance systems and out of pocket expenditures would be worthwhile. Panel data will be needed to analyze the direction of causality, however.
Institutional differences are probably also a source of the large differences in the use of health care services. For example, only 6% of the French and 8% of the German 50+ population has not visited any physician in the past 12 months, compared to 21% in Greece and 24% in Sweden. There is also significant variation in the proportions reporting in- or outpatient surgery, which varies from 7% in Greece to 14% in Germany.
SHARE also has some indicators of the quality of care, mainly based upon whether the physician asked about drugs, checked weight, etc. There are huge cross-country differences in the answers to these types of questions. Doctors in Greece seem to ask most questions; 38% of Greek respondents say their doctor asks about physical activity at every visit, compared to 6% in the Netherlands and 7% in Denmark. In Greece, 29% of respondents say their doctor checks their weight at every visit, versus 6% in the Netherlands or Denmark. Similar differences are found for whether the doctor asks about drugs or advises to get exercise (54% and 27% in Greece; 11% and 5% in the Netherlands). On the other hand, 73% of female respondents in the Netherlands have had a mammogram, compared to only 32% in Greece and 24% in Denmark.
2.7. Family Networks
The SHARE data show that the role of the family for the SHARE cohorts is quite strong. Between 70% and 80% of all respondents are from families with three or more living generations. There is a striking variation in regional proximity of the nearest living child across countries, with only 30% living less than one kilometer away in Sweden and Denmark, compared to around 70% in Spain, Italy and Greece. A similar north-south gradient exists for the frequency of contact with the most contacted child. For female respondents, the number of living children is negatively associated with education level in all countries except Sweden. This may be due to the traditionally excellent facilities for child care in this country, making it possible to combine work and motherhood at all occupational levels. There is a strong positive relation between frequency of contact and health limitations. Of those with no limitations in activities of daily living, 38% have daily contact with their most contacted child, compared to 50% for those with at least one such limitation.
Welfare systems have a strong impact on family transfers (Esping-Andersen 1990, 1999). The Nordic countries have a highly developed social protection system, whereas in the Mediterranean countries less welfare is provided through the State. Accordingly, more than 60% of SHARE respondents receive practical help from a child outside the household in Spain, Italy and Greece, compared to less than 45% in the other SHARE countries. In southern countries, help is mostly given within families. In Sweden, Denmark and the Netherlands, the help tends to take place between households.
While the fraction of grandparents who have looked after grandchildren at least once in the past twelve months lacks a north-south gradient and is similar in most SHARE countries (48% on average), grandparents who look after grandchildren do this more frequently in the southern countries. Among grandparents who have looked after their grandchildren in the past 12 months, less than 5% look after them on a daily basis in the northern countries compared to over 40% in the Mediterranean countries (as high as 55 per cent in Italy).
2.8. Well-being
SHARE has some indicators of the quality of work and the quality of life. Quality of work indicators can be used to construct indexes of effort, reward, and control. In terms of the effort-reward ratio, low quality of work is most prevalent in Italy and Greece (>50%) and least in Switzerland and the Netherlands (<30%). Low quality of work is significantly associated with mental health problems (as measured by the EURO-D scale) in five of the ten countries, without a clear north-south pattern. Low quality of work is associated with poor self-reported health in all countries.
To measure quality of life, SHARE uses an abridged version of the CASP-19 index, using 12 instead of 19 questions in the self-completion part of the questionnaire. The north-south gradient in this overall measure is again salient: the average value of the index (higher is better) varies from 33.4, 34.3 and 35.2 in Greece, Italy and Spain to 39.1, 39.8 and 40.5 in the Netherlands, All countries reveal a positive relation between well-being and education level and between well-being and income. The latter is stronger than the former. Overall, the average CASP index is 35.3 for the lowest 33% of the income distribution and 38.0 for the top 33%.
Salient cross-country differences exist for labor force participation and pathways to retirement. In the age group 60-64 for example, 31% report to be retired in Sweden, compared to 82% in Austria and 74% in France. Partial retirement (defined as retired but working more than 15 hours) is quite common in Greece and Switzerland (10%) but very rare in, for example, France (less than 1%). The latter may be explained by the fact that in France, combining earnings with a pension is usually not possible. Disability is an important alternative exit route in some countries but not in others. In the age group 50-65, more than 16% is on disability benefits in Sweden and Denmark, but only 3% in Austria and 4% in Greece. Eligibility criteria and generosity of the benefits system obviously plays a role here. See, for example, Bound and Burkhauser (1999) who compared disability transfer systems in the US, the Netherlands, Germany and Sweden and found that the systems have very different income effects that are consistent with the observed size of the system.
The intuition of "unused capacity" hinges on the incentives to retire early, embedded in social security and pension systems. However, other determinants of early retirement should be considered, for example health status. When considering only individuals who self-report to be in "good health" we find a strikingly high prevalence of people who report themselves fully retired in Austria, France and Italy. This is true even for people in early retirement (younger than 60). Further analysis shows that while health-related problems are one of the main reasons for retirement, there is a substantial proportion of retirees who report eligibility for retirement, early- or pre-retirement as a cause, particularly in Germany, the Netherlands and France.
2.9. Volunteer Work
A substantial fraction of the European 50+ population is engaged in volunteer work. In the Nordic countries, about 20% of the age group 65-74 does volunteer work, and in the Netherlands this is even more than 26%. Even among the 75+ volunteer work is done by about 12 or 13% in Denmark and Sweden. In Austria, Italy and Switzerland, volunteer work is rather common among the youngest age group (50-59) but less so among those past retirement age. In Spain and Greece less than 4% report to do volunteer work in all age groups. In all countries, volunteer work is much more common among the higher than among the lower educated.
2.10. Income, Consumption and Assets
The north-south differences that were salient in much of what was discussed above are also reflected in many of the main economic variables in the survey. Self-reports on how difficult it is to make ends meet show the largest differences more than 53% of couples in Spain, Italy and Greece find it difficult to make ends meet, versus 26% or less in all other countries. Financial wealth shows a similar difference median total financial wealth is much lower in the three Mediterranean countries than in all other countries. Somewhat surprising is the pattern of food consumption Sweden and Denmark have the lowest food consumption levels.
Substantial differences also exist in gifts and inheritances and intergenerational mobility of wealth. Large inheritances are predominantly found in Switzerland and Germany, where about 22% and about 16% ever received an inheritance of more than 150,00 euro, respectively, compared to only 6% in the Netherlands. This possibly relates to differences in taxation of inheritances.
Even though SHARE as a cross-sectional database already acts as a trove for new research findings, its full potential will only be realized once more waves are becoming available. After all, aging is a dynamic process and being able to paint a comprehensive picture of that process is the main aim of an enterprise like SHARE. Obvious examples of the advantage of panel data include the possibility to separate age and cohort effects, trends in health and retirement patterns, dynamics of the SES and Health nexus, etc. Perhaps the most important advantage is the possibility to gauge the effect of policy changes, both in the short run and the long run. By continually following representative samples in the different countries, one does not only have "before-and-after" measurements of a policy effect in a given country, one can also use the other countries as control groups.
3. Funding
Hitherto, there are three main funding sources: EU, NIA, and national sources in some countries. After the NIA grant through an IAG with UN ECE, funding was secured from the EU through two project proposals: SHARE and AMANDA ("Advanced Multidisciplinary Analysis of New Data on Aging"). In addition NIA provided two sources of extra support. Through an administrative supplement to the Health and Retirement Study, HRS expertise could be invoked in instrument design and interviewer training. Secondly through an IAG, this time with the World Health Organization, additional funds were made available to extend sample size and to add experimental modules with health and work disability vignettes (briefly described in Section 5 below).
Table 1 provides an overview of the funding sources of the first wave of SHARE. The largest part of the funding clearly comes from the European Commission for SHARE and AMANDA, for a combined total of about €5,750,000. The additional funding by NIA has been quite important however in aiding both quality improvement and in facilitating innovative experiments. National funding varies substantially. Belgium, Switzerland and Austria have completely financed their own surveys. As a non-member of the EU, Switzerland was not eligible for EU funding and has therefore provided its own funding. Belgium and Austria joined later, and hence were not included in the original grant applications. For the first wave, Sweden and Germany were the only countries that were able to secure additional funding from national sources.
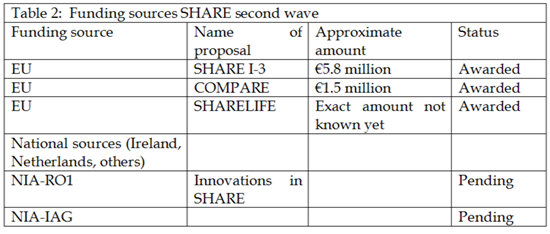
A second wave of SHARE is planned for the fall of 2006. Beginning in early 2005 a number of grant applications have been submitted to various funding agencies. Table 2 provides an overview of the various submissions and their funding status. Altogether, funding applications have been very successful, much more successful than could be expected merely on the basis of typical success rates of research proposals under the EU framework programs.
It is clear that a full blown SHARE in all countries of the EU requires a funding level and a long term commitment that exceeds the possibilities within the current framework programs. Securing funding for the first two waves has taken considerable effort from the SHARE researchers and the short-term nature of the funding so far (never more than for one wave) has made long term planning nearly impossible. There are encouraging signs that SHARE is gaining a status within Europe as a major source of information for policy and research regarding many interrelated aspects of aging. Acquiring that recognition is a major achievement of the group of SHARE researchers and in particular of the PI, Axel Boersch-Supan.
One might want to speculate what the effect has been of the uncertain funding situation on the quality of the data collected and on the speed with which the project got off the ground. In many ways constraints have forced the researchers to move more quickly and make less than fully informed decisions than would have been desirable from the sole viewpoint of data quality and response rates. On the other hand the pressure to show that SHARE is of great scientific and policy value has in a sense induced a nimble organization, where the players have shown to be able to produce under pressure. I would argue that despite the obvious downside to having to scramble for funds more or less continuously, the uncertain funding has done little harm. Now that SHARE has shown its viability and its importance as a source of new research, it should be easier to get long term funding. Were the uncertainty to persist, the effects might be a lot more detrimental however. The biggest danger of an uncertain funding situation would be the negative effect it has on attempts to work on continuous improvement of procedures and the stifling effect it may have on innovation
_Kapteyn.png)
Click the image to enlarge
4. Instrument Design, Implementation and Data release
Having both HRS and ELSA as role models, is a major advantage when it comes to instrument design and implementation. HRS and ELSA researchers are actively involved as advisors in SHARE; instruments and experiences are routinely shared between HRS, ELSA, and SHARE. Where originally the flow of know-how would be primarily from HRS to the younger siblings in the HRS family, increasingly flows of know-how go in both directions. Partly this is facilitated by the use of common interview software (Blaise or MMIC™, which is Blaise compatible). The close cooperation between the various projects furthermore helps to maximize comparability of data collected in the various countries, which facilitates internationally comparative analyses. This is one of the main motivations for implementing similar surveys in a large number of different countries as one can exploit the institutional variation across countries to better understand important topics. Examples include the following:
- Economic, social, and health-related determinants of retirement, including partial and phased retirement, and alternative exit routes such as unemployment and disability;
- Well-being, health, and time use of the elderly in different countries;
- Determinants of obesity, including lifestyle, institutions, and socio-economic status (SES). Changes in health and socio-economic status and the role of institutions.
Some descriptive analyses along these lines were summarized in Section 2 above.
Designing an instrument for eleven countries poses a number of major challenges. One needs to agree on the content of the survey; then design it in such a way that justice is done to institutional differences, while at the same time maintaining comparability of the collected data. On top of that, the instrument needs to be translated in the languages of the different countries. The structure chosen for this is roughly as follows:
- The questionnaire is divided up in a number of modules. Each module is the responsibility of a working group, typically consisting of researchers from different countries.
- Proposals by working groups are submitted to the central management team at MEA, Mannheim University, and discussed at plenary meetings where all working groups and countries are represented.
- The resulting draft instrument is programmed by CentERdata (the institute responsible for the technical coordination and implementation) in English.
- After a number of experiments and pilots, the instrument is translated into the various languages (fourteen at the moment , using a "Language Management Utility' (LMU). The generic setup of the Blaise files results in datasets having a common structure across countries. Question texts, interviewer instructions, answer categories, etc. are stored in one common database. The LMU is meant to manage the different languages in that database. By using the database a language specific instrument can be created rather quickly. See Das, Vis, and Weerman (2005) for more details. A brief summary of the translation process, taken from Das, Vis, and Weerman (200) is as follows:
"the set-up of the CAPI instrument was generic: the routing in the instrument was fixed, and only texts were changed from country to country. These texts were stored in a database, and in order to fill the database, CentERdata developed a so-called Language Management Utility (LMU). The LMU was not intended as a helping device for translators, but made the creation of country specific CAPI instruments possible in a very short period of time, parsing translated texts into a country specific instrument based on the blueprint of the generic version. Another program was developed to process a paper version of the individual country specific CAPI instruments, based upon the generic routing and the country specific texts in the LMU database.
The SHARE LMU could be accessed via the Internet. After entering a country specific username and password, the main screen was shown… For countries using more than one language in SHARE (Switzerland and Belgium) a dropdown menu with a language selection appeared. This dropdown menu was not visible for other countries.
Once a translator had selected a module in the screen… and had clicked on 'View', a listing of all questions in that particular module was shown. Here the translator could select a question to translate. For all questions the generic (English) text was shown first, followed by the translated text. At the end of the listing of all questions an option for viewing all questions for that module was given. This was in particular helpful when checking all translations. Standard answer categories (like 'yes'/'no') had to be translated only once."
"There were only a few ways to bypass the generic blueprint of the questionnaire, introducing country specific routing. First, in a few (exceptional) cases the generic routing tested for a condition based on a variable containing a country specific code, affecting the generic routing. This was used in sections that differ quite a lot across countries, like e.g. the health care section. Second, country specific elements could be introduced by skipping irrelevant answer categories, and adding new country specific answer categories in the LMU. However, because of the generic set-up of these new answer categories, this never led to a different sequence of questions for one specific country." - Once the translation is found to be satisfactory, one final pilot takes place in all countries involved. After evaluating the results of the pilots in all countries and making necessary final adjustments, the final instrument is fielded in the participating countries by local survey agencies.
The translation process aims at combining the requirement of a common structure of the dataset, which is essential for cross-country analyses, with sufficient flexibility to allow for institutional differences (e.g. in the pension system). This does not address the deeper issue of cross cultural comparability of responses. It is clear for instance that the meaning of a term like "excellent health" carries different meanings in different countries. SHARE has spawned a veritable cottage industry of research delving into methods to somehow making these terms comparable. Prime approaches are the use of vignettes (as explained below) and the use of objective physical performance measures, like grip strength. This is an area where the collection of biomarkers holds particular promise.
The role of the national survey agencies merits a brief description. Following the European and national rules for procurement, the agencies are selected within each country by the relevant country team, based on a tender among at least three competitors. The agencies do the sampling and carry out the fieldwork within narrowly described guidelines drawn up centrally. All agencies use the instrument programmed in Blaise; a centralized sample management system developed by CentERdata is used in all countries and provides bi-weekly feedback on the progress of the fieldwork in each country. Data are sent to CentERdata every two weeks converted to SPSS and STATA files and posted on an internal web-site.
The coordinated fieldwork allows for quick data release. For the first wave, fieldwork started in May 2004 and ended in October. By the end of November data for most countries were accessible in a central database at CentERdata. A database management team has provided imputations and checked consistency of the data. The official first release of the data was made available to the research community in April of 2005. Concomitant with the release of the data a first results book was published with mainly descriptive analyses by the project's researchers (see Section 2 above). A first conference with early results took place early October 2005, in Lund, Sweden.
5. The Secret of its Success
The title of this section suggests that I believe SHARE to be a success already. Indeed I do. It is always hard to apportion success to different causes. In somewhat arbitrary order I list a number of important points, which I believe to have contributed to SHARE's success so far.
- SHARE is research driven and researcher managed. Following the lead of HRS, SHARE is under complete control of the researchers involved. This has several implications. (1) Since researchers design the questionnaires, these are guaranteed to address research questions scientists care about; (2) Researchers have an interest in having the data available soon and in a manageable format, which facilitates quick release of newly collected data ; (3) Related to the first point, new scientific developments are incorporated quickly in questionnaire content, because researchers have an interest in following scientific developments; (4) the multidisciplinary nature of the survey instrument provides a natural meeting place for researchers with different backgrounds to work together.
- The strategic role of NIA and U.S. researchers. None of the points made above is new, but their merit was demonstrated by HRS in a more powerful way than ever before in the social sciences. As indicated in Section 2 above, U.S. researchers involved in HRS played a crucial role in getting SHARE started. By bringing a group of good researchers from Europe together with the major U.S. researchers in aging and by providing seed money to start planning an HRS in Europe, NIA and the U.S. researchers played a key role in getting SHARE off the ground.
- Flexible informal organizational structure. This is an advantage, at least under the condition of strong leadership.
- Leadership role of the Principal Investigator. SHARE is a complex project in many different respects: many institutions; many countries; many disciplines; fieldwork to be done by separate organizations in the participating countries. Without strong leadership a project of this complexity would not be possible. Both the personal leadership of the PI and the support team at MEA are crucial success factors. In a sense this makes SHARE vulnerable, as so much depends on only a few key people, but at the moment the benefits far outweigh the risks.
- Common technical infrastructure. Given that surveys are done by local agencies, a possible choice could have been made to let each agency use its own software and thus to some extent let each agency implement its own instrument. In contrast SHARE has adopted a model of one technical infrastructure where all programming is done centrally and where also sample management is in the hands of a central organization. The institute responsible for the technical design and implementation, CentERdata (http://www.uvt.nl/centerdata/en/) has proved invaluable in the implementation of this strategy.
- Open and eclectic research philosophy. Like HRS and ELSA before it, SHARE is not focused on one particular research hypothesis or wedded to one particular paradigm. On the contrary, SHARE is eclectic by design. The core instrument is meant to accommodate a wide swath of potential research topics, covering various disciplines. In addition to the core instrument several mechanisms facilitate experimentation and the exploration of new research directions. One mechanism is the addition of modestly sized samples, which are given the core instruments, but in addition are asked special questions in certain domains. For example, in six countries -Sweden, Greece, Spain, Germany, the Netherlands and Italy- vignette questions were fielded in the late fall of 2004, after the main survey. France and Belgium followed later. These vignettes were part of drop-off left behind with respondents after they had completed the main (core) SHARE questionnaire. The sample size in each country was on the order of 500 respondents. This sample is an addition to the core SHARE sample and thus the experiment has the added value of increasing sample size of SHARE in the countries that decided to participate in the vignette experiments. In total 18 vignettes on six domains of general health (3 vignettes in each domain), pain, mobility, sleep, cognition, depression, and breathing were administered. These domains were selected on the basis of self-reported health and vignettes in different surveys in the Netherlands (CentERpanel) and several other European countries (World Health Survey), where it was found that, first, response scale differences in these domains were important and, second, these domains contributed most to overall self-reported health. In addition respondents were given 9 vignettes on three domains of work disability (pain, depression, and cardiovascular disease).
6. The Future of SHARE
As the cliché goes, forecasting is difficult, particularly of the future. I believe there are reasons to be optimistic about SHARE's future. The current momentum makes structural funding increasingly more likely. Ideally most of this funding should come from the European Union. Central funding is important to provide incentives for coherency in questionnaire content and data dissemination across countries. On the other hand, an increasing number of countries at this moment already completely self-finance their part of SHARE or provide substantial co-funding, as pointed out in Section 4.
When reflecting on the future of SHARE, the most interesting part is to speculate on new scientific directions the enterprise may take. In many ways the HRS is a good model here. HRS has evolved from a major data collection effort into a virtual laboratory in which several experiments are taking place. Increasingly researchers propose to do additional studies involving HRS respondents, taking advantage of the rich information already available about the HRS respondents. An example is the ADAMS study (Aging, Demographics, and Memory Study), which conducts in-home clinical dementia assessments in a sub-sample of 856 HRS respondents aged 70 years or older. The HRS sample provided the sample frame for the ADAMS where the sample was stratified based on cognitive status. Another example is the Consumption and Activities Mail Survey in 2001 with follow-up waves in 2003 and 2005 (and new ones planned in 2007 and beyond). For a random subset of HRS households, CAMS obtains a complete measure of spending. In combination with the already available information on wealth holdings and income, this provides a very complete picture of the economic well-being of households.
Similar developments are taking place in SHARE. A defining characteristic within SHARE is that experiments may vary by country and that many experiments are performed in several, but not all, participating countries. For instance, the experiment with work disability and health vignettes drop offs in the first wave was carried out in 8 of the original 11 SHARE countries. The variation across countries may reflect different views among country teams of the desirability or feasibility of doing certain experiments in their countries. For the second wave a number of new experiments is planned, including vignettes for other life domains than health, the measurement of life histories and experiments to improve response rates. For more advanced experiments, e.g. the collection of biomarkers or links to administrative data, differences in legal framework will probably induce substantial differences in what will be done. There is nothing wrong with that. Doing some experiments in a few countries only may inform other countries about its feasibility or usefulness. There is no need to perform every experiment on a European scale from the start. On the other hand, one would hope and expect that successful experiments in some countries will increase the attractiveness of doing the same experiments in remaining countries. In that sense the dynamics within SHARE will not be different of the dynamics across HRS, ELSA, SHARE, MHAS, and other similar projects. Each of these projects learns from the others.
What are the most obvious new developments we could expect? I mention a few:
- More countries: Starting from the original 11 countries, SHARE now comprises 15 countries, including two from Eastern Europe. I would expect the number of countries to keep increasing, thereby adding to the value of the exercise in all countries. By increasing the number of countries, studies of the effect of policies and institutions on outcomes become more powerful and hence the addition of another country also adds to the value of the information collected in the currently participating countries.
- Collection of physical performance measures, including biomarkers. This is an example of a development that is unlikely to take place synchronically in all countries, due to different infrastructures, legal restrictions and levels of experience and sophistication of survey agencies.
- Links to administrative data. The Scandinavian countries have a long tradition of building and maintaining large administrative databases that can be used for micro-analyses. A promising development is the linking of these databases to survey information. In a recent project between the University of Uppsala and RAND we have drawn respondents from LINDA, an administrative database in Sweden and linked survey information to administrative information. This allows for at least two important types of analysis: cross validation of different sources of information (e.g. income available in the administrative database and income collected in the survey, see Kapteyn and Ypma, 2005) and combining administrative data with information not typically available in such databases (e.g. subjective health). The latter aspect provides a genuine extension of analytical capabilities. For instance, one can link current survey information to administrative information going back in time and thus substantially expand the information set available for analysis. Statistics Netherlands is currently running a pilot experiment with the institute Netspar at Tilburg University, in which survey data collected by researchers are given to Statistics Netherlands, which organization then links these to administrative data. The SHARE data are a prime candidate for such a procedure. Due to data protection considerations use of the linked data is more restrictive than the use of just the pure survey data, but it appears that a fairly flexible and practical modus has been worked out.
- Additional experiments and the use of different modes. This would follow the HRS example, where the context of SHARE is used as a virtual laboratory in which additional experiments have a high pay-off in view of the information that is already available about the respondents. Furthermore, with changing technology, an obvious approach is to vary the mode of data collection, depending on the type of data one is collecting and the goal of a particular experiment. For example, CentERdata has received a large grant to set up a representative household panel of 5000 households. The panel is representative in the sense that population registers serve as a sampling frame and that potential respondents who do not have Internet access will be given the necessary equipment to be able to browse the Internet and send and receive emails. All households in the panel will have high speed Internet. The Internet panel is used for a variety of experiments and for the longitudinal collection of data on a wide spectrum of topics, taking advantage of the fact that lengthy questionnaires can broken up into small pieces so that respondent burden within any given period is kept low. Part of the information collected will be the SHARE core instrument, thus effectively doubling the SHARE sample size in The Netherlands from about 2000 households to about 4000. The households in the Internet panel will also be asked to provide additional information, including biomarkers and data that may be collected through experience sampling. Experiences with the collection of this type of information over the Internet can then next be used to inform SHARE as a whole of its feasibility and merits.
7. Concluding Remarks
SHARE is the result of a number of fortuitous circumstances: powerful examples set by HRS and ELSA, well-timed initiatives by U.S. researchers and the strategic role played by NIA, a committed PI with an equally committed staff, a survey research institute with the technical capabilities and the energy to pull it all together. One question one may nevertheless ask is: if we were to do it again, would we want to do things differently? At one level the answer to a question like that is always in the affirmative. Some procedures could have been streamlined a bit more, a somewhat longer field period would have raised the response rates a little higher, etc. But I believe that given the constraints under which SHARE had to be put together, in broad outline one would want to follow the same strategy again. An enterprise like SHARE is an adventure rather than a tightly planned process. Flexibility and the willingness to adjust to new events or insights are essential ingredients.
 Click on the PFD icon above to download the entire paper
Click on the PFD icon above to download the entire paper